


The landscape of Medicaid reimbursement for nursing homes is undergoing significant changes. Presently, eight states have adopted the PDPM case-mix index (CMI) model, and an additional 31 states are set to follow suit over the next two years.
This shift is primarily motivated by the alterations to the MDS, particularly the removal of Section G in October 2023. This change necessitated the transition to PDPM CMI, because RUG-based CMI calculations are unfeasible without Section G.
While this information may not seem particularly noteworthy at first glance, its significance becomes apparent when considering the downstream implications, particularly in terms of staffing adjustments and quality measures.
In essence, the adoption of PDPM Medicaid CMI is poised to alter the patterns of assessment data capture in the states that have embraced this transition.
The provocative nature of the last sentence is intentional. Historical transitions in payment systems over the past few decades have consistently resulted in shifts in MDS data capture patterns. Explanations for these shifts generally fall into two categories: Either providers are strategically adjusting their practices to maximize reimbursement, or the increased focus on specific MDS items is leading to more accurate assessments. Throughout my career, I’ve found myself in both camps, but as I’ve matured, I’ve come to appreciate the one with a clearer view and running water!
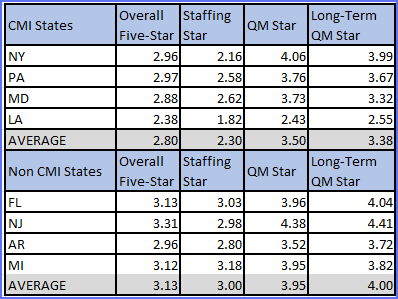
All jests aside, my suspicion is that states transitioning to PDPM CMI reimbursement may experience a downgrade in Staffing and Quality Measure Five-Star ratings. In today’s reimbursement environment, disparities exist in these two Five-Star domains based on the state in which a facility is operating and that state’s Medicaid reimbursement system. Considering these factors is important when evaluating the quality of care in nursing homes using the Five-Star rating system.
The table below illustrates the statistically significant differences in Five-Star scores between states that are CMI Medicaid reimbursement and those that are not. In this example, we analyzed quarter three of 2022. (CMI states were then using RUGs and not PDPM.)
In April, CMS is set to enact a temporary freeze on the Staffing domain of the Five-Star rating system. By July, this freeze will be lifted, revealing a new staffing adjustment methodology. While the specific details of this adjustment are yet to be disclosed, we know it will be based on the PDPM nursing category and the average CMI for this section. Notably, this same section is increasingly influential in driving Medicaid reimbursement in numerous states.
CMS has assured providers that they will “revise the staffing rating thresholds to maintain the same overall distribution of points for affected staffing measures” (see their QSO-23-21-NH memo). Essentially, this commitment implies that the national average numbers of nursing homes with 1- , 2- , 3-, 4- , and 5-star Staffing ratings will remain unchanged. However, at the provider level, significant movement is expected, including a systematic decline in the new CMI states. This adjustment underscores the dynamic nature of the healthcare landscape and the need for providers to adapt to evolving methodologies and criteria.
In preparation for the impending shift, I turned to my esteemed colleagues at Zimmet Healthcare Services Group (ZHSG) for insights. In their analysis, they provided a valuable look at how the nursing category distributes in the initial quarter of a state’s transition to PDPM CMI Medicaid reimbursement. This foresight will undoubtedly prove instrumental in navigating the nuances of the changing landscape, allowing us to proactively address challenges and optimize our approach during this transitional period. Collaboration and shared expertise within our team at ZHSG are essential resources as we navigate the intricacies of evolving healthcare policies and methodologies.
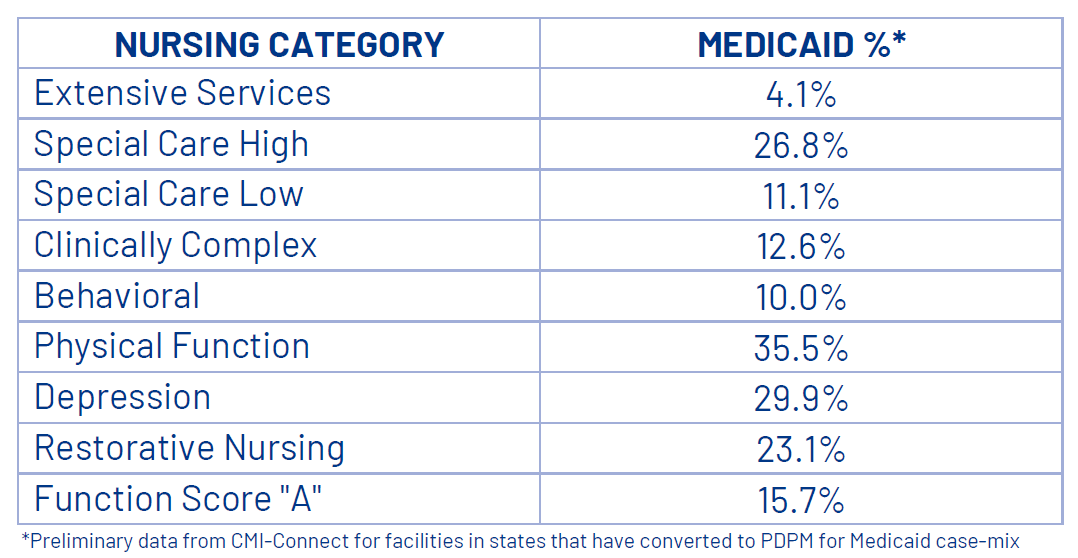
Vincent Fedele, partner at ZHSG and chief operating officer for CMI-Connect, shared these thoughts: “Most interesting within the early data is how much potential exists within the critical Special Care High category. There is a wide variance from top-performing nursing homes to the rest of the pack. Most of these differences can be explained by their strategy and capture and not the acuity of the resident population.”
He continued: “Also noteworthy is the Function Score ‘A’ capture that is 10 times higher than what we see within the short-term Medicare population. This is significant as ‘independent’ function scoring will often result in the resident classification falling from one of the higher-paying categories to the lower Clinically Complex category, reducing CMI in the process.”
But how will these initial findings evolve in the coming years? On the topic of reimbursement systems, I leveraged the deep expertise of both Vincent and Michael Sciacca, also a partner at ZHSG. The insights they provided proved to be fascinating. Their analysis likely offers a valuable glimpse into the future landscape, enabling us to strategically plan and adapt our approach in alignment with the expected trends and challenges.
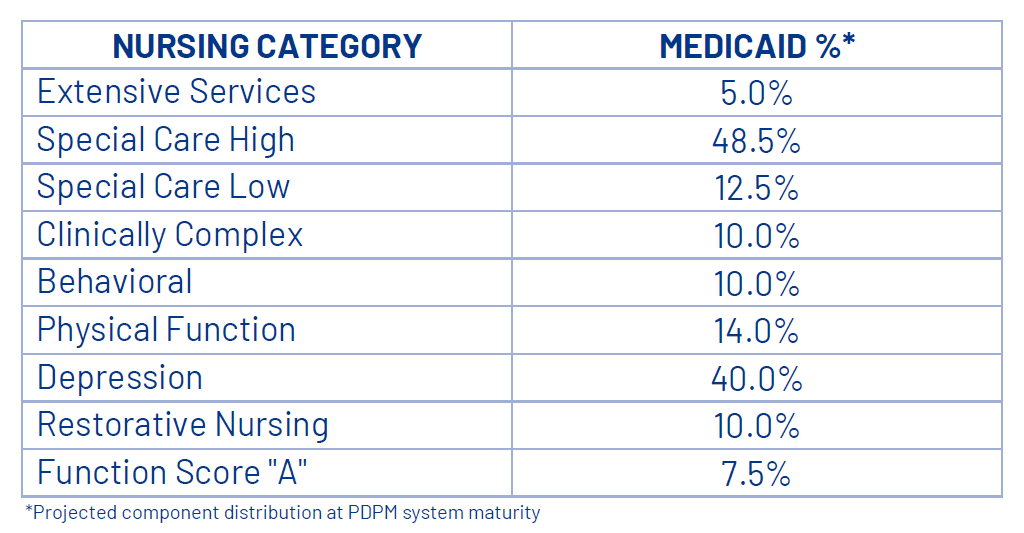
Mike shared: “We will continue to see migration from the lower Physical Function and Behavioral categories to the Special Care categories in large part due to the identification and capture of applicable clinical acuities. We expect Special Care High category capture to top out at close to 50% of all resident days. Improvement in interview/staff assessment will help with the capture of mood items and the Depression end split. This expected creep will take some time, but operators have already put in place comprehensive policy and procedures to ensure appropriate documentation related to these acuities.”
If the predictions from Vin and Mike prove accurate, the anticipated upward movement in the distribution of nursing categories will likely result in increased resident acuity for providers, necessitating a higher staffing level. Without it, the adjusted Staffing domain ratings are expected to decline. This presents a notable challenge, particularly when attracting and retaining staff is already a significant concern for providers. The impending staffing mandate emphasizes the need for strategic workforce planning and retention initiatives within the healthcare industry. Navigating these challenges will require a proactive and comprehensive approach to staffing management.
Predicting the trajectory of the Quality Measure domain poses a greater challenge. Substantial movement is expected across all facilities due to changes in the definitions of certain quality measures. Notably, the risk adjustment for long-stay pressure ulcers has been removed, which will lead to the wrong conclusion of a worsening industry-wide trend. Additionally, the scope of the bowel and bladder incontinence quality measure is expanding beyond low-risk residents, potentially triggering more residents; however, it now focuses solely on new or worsening incontinence incidents.
The other activities of daily living measures within the Five-Star rating system present a unique set of challenges, making it difficult to anticipate their impact. In past transitions, such as Connecticut’s shift to MDS-based CMI Medicaid reimbursement in July 2022, a noticeable drop in long-stay quality measures was observed. In this instance, Connecticut experienced an average decline of one star in the Quality Measure domain during the transition. This historical pattern may offer some insight into what could transpire in other states undergoing similar changes, but the nuanced nature of quality measures makes precise predictions challenging. Vigilance and adaptability will be crucial in managing the potential fluctuations in the Quality Measure domain.
My most crucial advice extends beyond a simple “be careful.” Recognize that navigating changes in reimbursement systems and quality measures is a serious matter. While it may at times feel like a game of Whac-a-Mole, deliberately manipulating your MDS for artificial financial or quality gains will inevitably manifest in your data and, more significantly, impact the care you provide.
I strongly advocate for a focus on precise assessment, meticulous care planning, effective care delivery and thorough evaluation. By prioritizing these fundamental aspects, you are poised to achieve the desired results authentically. This approach not only safeguards against potential pitfalls but, more importantly, contributes to delivering genuine and high-quality care to your residents.
Steven Littlehale is a gerontological clinical nurse specialist and chief innovation officer at Zimmet Healthcare Services Group.
The opinions expressed in McKnight’s Long-Term Care News guest submissions are the author’s and are not necessarily those of McKnight’s Long-Term Care News or its editors.
Have a column idea? See our submission guidelines here.





