


The headlines in the NY Times, Wall Street Journal and other publications say it all:
- “Candida Auris: The Fungus Nobody Wants to Talk About”
- “A Mysterious Infection, Spanning the Globe in a Climate of Secrecy”
- “Outbreaks of Untreatable, Drug-Resistant Fungus Spread in 2 Cities”
- “The Last of Us: Fungal infections really can kill – and they’re getting more dangerous”
In my conversations across the nation, I have asked many leaders what they are doing to prevent the introduction or spread of this emerging fungus. Most leaders defer to their infectious disease expert, and some asked me what the big deal is about it. As one person said, “It is just a fungus.”
Yes, it is a fungus, but it is a deadly one and does not play by the rules of expected fungal behavior. So here is what we know about Candida auris:
- First recognized in 2009 in a 70-year-old individual with external otitis in Japan
- Retrospective review of strain collections found the earliest known strain back to 1996 in South Korea
- Following the first isolation in Japan, cases have been reported in several countries on five continents. Although uncommon for fungi, C. auris has caused outbreaks in India, the United Kingdom, Spain, the United States, Venezuela, Colombia and South Africa
- As of 2022, C. auris isolates have been identified in most countries and continents except for Antarctica
What allows C. auris to thrive and survive more efficiently than other Candida species?
Here is what we know:
- It grows well at high temperatures. Other Candida species tend to be destroyed at high temperatures.
- It can withstand high salt concentrations. This also prolongs its survival.
- It is resistant to common antifungal medications, which makes infections difficult to treat.
- It requires special lab methods to identify it as the source of infections. Most labs are not equipped to detect Candida auris, resulting in misidentification and the wrong treatment.
- C. auris is the first human pathogenic fungus to be subject to international health alerts because of its propensity to colonize skin, persist in the healthcare environment, cause nosocomial outbreaks, and severe disease.
One of the fascinating traits linked to C. auris’ emergence as a nosocomial pathogen is its ability to persist in healthcare settings on surfaces in the face of stringent cleaning protocols. It is resistant to most commonly used disinfectants.
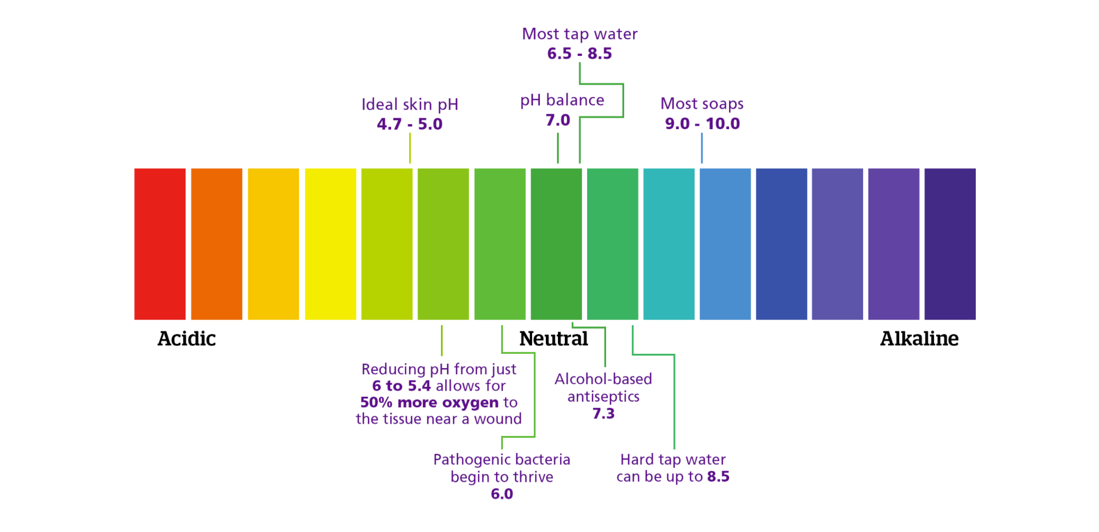
Candida auris does have an Achilles heel. It cannot reproduce and survive in an anaerobic or acidic environment. Skin needs a low acidic pH to be able to be the first line of defense against the colonization of pathogens. Yet, skin’s ability to be that defense is severely impeded daily. Table 1 shows how bathing with soap and water changes the pH of the skin, which enables growth of pathogens.
Table 1: The Impact of Daily Actions on the pH of the Skin
In my research, I found a novel topical that can be used in the fight against Candida auris. The ingredients are safe to use on mucosa, which is at high risk for colonization of the fungus. Invitro studies showed the efficacy of the ingredients against Candida auris with reductions of 83% to 99% over a 4-8-24 hour period. A low acidic sustained skin pH creates a hostile environment against pathogens, including Candida auris.
In the fight against pathogens such as Candida auris, we must rethink our actions and use Candida auris’ Achilles heel to our advantage. #pHMatters
Martie L. Moore, MAOM, RN, CPHQ, is the President/CEO of M2WL Consulting. She has been an executive healthcare leader for more than 20 years. She has served on advisory boards for the National Pressure Injury Advisory Panel and the American Nurses Association, and she currently serves on the Dean’s Advisory Board at the University of Central Florida College of Nursing and Sigma, International Honor Society for Nursing. She was honored by Saint Martin’s University with an honorary doctorate degree for her service and accomplishments in advancing healthcare.
The opinions expressed in McKnight’s Long-Term Care News guest submissions are the author’s and are not necessarily those of McKnight’s Long-Term Care News or its editors.





