


Imagine for a moment being trapped in your own mind.
Unable to form words, unable to understand others.
Unable to successfully have your most basic needs met.
For individuals with aphasia, this is how they often feel. I imagine it is terrifying.
It robs individuals under its grasp of the ability to communicate. It impairs their capability to gather thoughts and can limit their skill in understanding others.
Type, presentation and severity are largely based on localization of damage within the brain.
According to the American Speech Language Hearing Association (ASHA) aphasia is an acquired neurogenic language disorder resulting from an injury to the brain — most typically, the left hemisphere. Aphasia involves varying degrees of impairment in four primary areas:
- Spoken language expression
- Spoken language comprehension
- Written expression
- Reading comprehension
Depending on an individual’s unique set of symptoms, impairments may result in loss of ability to use communication as a tool for life participation (Threats & Worrall, 2004).
A person with aphasia often has relatively intact nonlinguistic cognitive skills, such as memory and executive function, although these and other cognitive deficits may co-occur with aphasia.
Common causes of aphasia include the following:
- Stroke
- Ischemic — caused by a blockage that disrupts blood flow to a region of the brain
- Hemorrhagic — caused by a ruptured blood vessel that damages surrounding brain tissue
- Traumatic brain injury
- Brain tumors
- Brain surgery
- Brain infections
- Progressive neurological diseases (e.g., dementia)
Stroke is the most common cause of aphasia. According to the National Aphasia Association (n.d.), about 25% to 40% of stroke survivors experience aphasia. Approximately 35% to 40% of adults who are admitted to an acute-care hospital with a diagnosis of stroke are diagnosed with aphasia by the time they are discharged (Dickey et al., 2010; Pedersen, Jorgensen, Nakayama, Raaschou, & Olsen, 1995).
Diagnosis and treatment of aphasia require detailed testing, assessment, patience, and a skilled care provider with an understanding of appropriate evidence-based practice to advance function.
And then there is the CODING!
MDS Accuracy
ICD-10
Remember, aphasia and coding accuracy has a significant impact on PDPM related to co-morbidity for speech language pathology (SLP).
National trends related to SLP continue to show a significant volume of “SA” (i.e. no PDPM criteria identified and coded on the MDS).
As a result, I thought for today we would consider coding practices for aphasia.
Recall-CMS noted this to be a trending area associated with historical SLP needs, so let’s do our due diligence in understanding its impact on those we serve.
Consider a case study:
Perspective, Mrs. Adams (patient):
I arrive at your skilled nursing facility following a long hospital stay. Everything is new. I can hear your words. I can see your mouth moving. I struggle. Nothing makes sense.
I miss reading the morning paper.
I miss talking to my daughter on the phone.
My words “stick” in my head or worse they “stay”, and I repeat myself over, and over, and over.
They say I had a stroke.
Aphasia makes it hard for me to communicate.
Perspective, Sharon, MDS Coordinator:
Mrs. Adams is complex. Review of these medical records will take a significant amount of time. All the testing, instrumental studies, radiology reports …. and we need to have a way to understand her.
Aphasia, her discharge summary includes a diagnosis of aphasia- but which ICD-10 code should I use??
First, I am going to review my RAI Manual.
Certain portions of Section I: Active Diagnoses in the Last 7 Days allow Aphasia to be coded in I4300 and others require entry in I8000 including codes within the “I69” series which provide specificity associated with type of cerebrovascular impairment or disease.
| Speech and Language Deficits | I69020 | Aphasia following nontraumatic subarachnoid hemorrhage | ||
| Speech and Language Deficits | I69120 | Aphasia following nontraumatic intracerebral hemorrhage | ||
| Speech and Language Deficits | I69220 | Aphasia following other nontraumatic intracranial hemorrhage | ||
| Speech and Language Deficits | I69320 | Aphasia following cerebral infarction | ||
| Speech and Language Deficits | I69820 | Aphasia following other cerebrovascular disease | ||
| Speech and Language Deficits | I69920 | Aphasia following unspecified cerebrovascular disease |
I also have to meet the definition of “Active” — ACTIVE DIAGNOSES are physician-documented diagnoses in the last 60 days that have a direct relationship to the resident’s current functional status, cognitive status, mood or behavior, medical treatments, nursing monitoring, or risk of death during the 7-day look-back period.
Furthermore, if aphasia is an impairment in language, I should likely see impairments documented in Section B: Hearing Speech and Vision.
Specifically, B0700: Makes Self Understood and/or B0800: Ability to Understand Others.
Impairments in one area or the other will likely align with the specific classification of aphasia. I will work with Marco, our SLP to determine type and severity.
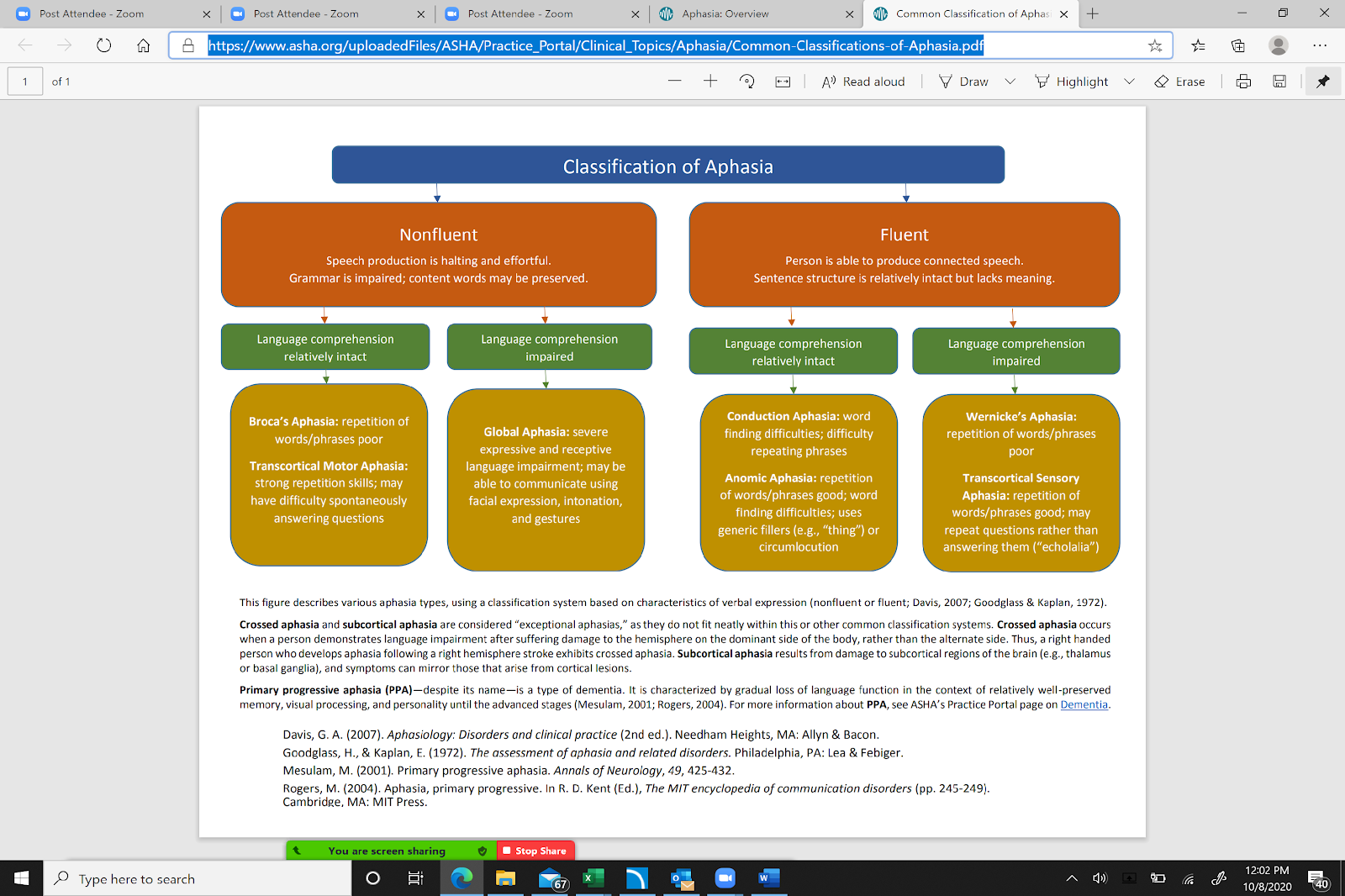
Source: American Speech Language Hearing Association; Classification of Aphasia
Perspective, Marco, Speech-language pathologist:
Mrs. Adams has aphasia, it’s complex and appears to align with Broca’s type, she repeats often.
Perseveration.
Her words are effortful, but she is stimulable for interventions including pacing.
She enjoys singing per her family. Perhaps Melodic Intonation Therapy (MIT) will be a beneficial approach.
Do not worry, Mrs. Adams
We know you feel stuck in your own head.
We are here and we will help you find your words again!
Renee Kinder, MS, CCC-SLP, RAC-CT, is Executive Vice President of Clinical Services for Broad River Rehab and a 2019 APEX Award of Excellence winner in the Writing–Regular Departments & Columns category. Additionally, she serves as Gerontology Professional Development Manager for the American Speech Language Hearing Association’s (ASHA) gerontology special interest group, is a member of the University of Kentucky College of Medicine community faculty, and is an advisor to the American Medical Association’s Relative Value Update Committee (RUC) Health Care Professionals Advisory Committee (HCPAC).





