


Clear but heavy. Like clear glass hitting just below the surface. Depression in the elderly.
There is a level of neurosis in my bones around routine that occurs twice daily.
Precisely in the morning after the kids leave for school and in the evenings after they go to sleep.
The a.m. routine involves making all the beds in the house. It’s an obsession, an art actually in my opinion when done correctly, one I cannot let go, and one that has to be complete before I can start my day.
The p.m. routine is more about the residual dish overload.
As I am writing this, my evening roundup, and this is after supper, included finding a coffee cup full of some form of hot chocolate creation, multiple bowls with leftover morsels of Lucky Charms cereal, a saucer with six6 egg yolks because Joseph’s go-to after school snack is boiled eggs but only the whites, a “snackie” with stale goldfish and water, and a plate with one full piece of bacon and a regurgitated bite of fried pork chop.
Can’t make this stuff up.
And then, just when I think I am in the clear, I see it. A cup of water and bubbles on a bathroom countertop.
Arghhh.
I walk to the kitchen, pour what I assume was water and bubbles into the kitchen sink — without the strainer — and suddenly I hear a bizarre noise.
Like heavy glass, “clunk, clunk, clunk.” As the bubbles clear, I see the culprit.
Clear marbles from the Kerplunk game.
Just below the surface, and completely unnoticed, the cup had been full of marbles. I proceeded to run water and pick each one out.
Amazingly, that while clear, they all have small ribbons of color, blues, and reds, and greens; however, when disguised by the bubbles, I never knew they were lingering.
I think in this moment. Is this why we struggle to appropriately identify depression in the elderly?
Is it just below the surface? Left unnoticed? Or simply not properly assessed?
Recent news publications including a new survey of 365 nursing home residents in 36 states, conducted in July and August by the nonprofit Altarum Institute, shows that pandemic restrictions have affected nearly every part of the lives of those residing in skilled nursing facilities, especially their mental health.
The survey was distributed nationally as an online, public link and the following statements where noted:
“Being restricted for six months is a very big percentage of their remaining lifetime and very obviously devastating,” stated Anne Montgomery, co-director of Altarum’s Program to Improve Eldercare
The following comments were also noted by residents surveyed:
“If the virus doesn’t kill me, the loneliness will.”
“I have become more anxious and depressed due to the separation from loved ones.”
And, “I have little appetite and am losing weight.”
For those of you tirelessly working in skilled nursing facilities daily, these statements will likely not come as a surprise.
These comments so raw, so true. But I wonder: If these people were not surveyed in the right way, would we have these insights?
Or would they continue to sit inside, unnoticed or accounted for?
All the window visits, FaceTime connections, and hug machine contraptions in the world do not take the place of true human contact and extended visits with families.
With that said, our key priority now is keeping everyone safe.
What I am here to ask today is that we improve our metrics for early identification, testing and care planning for depression.
Why? Well, because what we know to be true is not aligning with the data reported to the Centers for Medicare & Medicaid Services, as depression impacts the Patient Driven Payment Model.
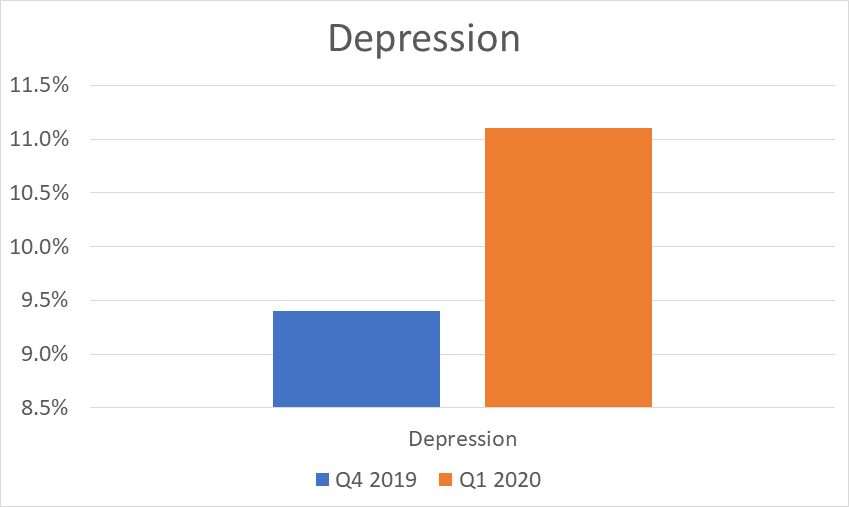
Take, for example, what’s below, which provides a national view from the CMS Research Data Assistance Center (ResDAC) regarding trending for reported depression for Medicare Part A beneficiaries Q42019 to Q12020. Based on the below, only about 11% of individuals would meet the criteria in the first quarter of 2020.
Anecdotal reports, research and just plain common sense tell us that the rates should be much higher.
Source: CMS ResDAC PDPM Depression % National Q42019 versus Q12020
As with all assessment protocols included in the Minimum Data Set, start with your RAI Manual. Specifically, the criteria in Section D for Mood and clinical practices for D0200: Resident Mood Interview (PHQ-9©) and D0500: Staff Assessment of Resident Mood (PHQ-9-OV©).
Remember, the resident qualifies for depressed if D0300 is greater than or equal to 10 but not 99; OR D0600 is greater than or equal to 10.
Section D Mood Intent:
The items in this section address mood distress, a serious condition that is underdiagnosed and undertreated in the nursing home and is associated with significant morbidity.
It is particularly important to identify signs and symptoms of mood distress among nursing home residents because these signs and symptoms can be treatable. It is important to note that coding the presence of indicators in Section D does not automatically mean that the resident has a diagnosis of depression or other mood disorder.
Assessors do not make or assign a diagnosis in Section D; they simply record the presence or absence of specific clinical mood indicators. Facility staff should recognize these indicators and consider them when developing the resident’s individualized care plan.
Depression can be associated with:
* psychological and physical distress (e.g., poor adjustment to the nursing home, loss of independence, chronic illness, increased sensitivity to pain)
* decreased participation in therapy and activities (e.g., caused by isolation)
* decreased functional status (e.g., resistance to daily care, decreased desire to participate in activities of daily living [ADLs]), and
* poorer outcomes (e.g., decreased appetite, decreased cognitive status).
Findings suggesting mood distress should lead to:
* identifying causes and contributing factors for symptoms
* identifying interventions (treatment, personal support, or environmental modifications) that could address symptoms, and
* ensuring resident safety.
In closing, one should consider:
What are your rates internally for a person’s identified depression?
Who is part of the team identifying the risk for depression?
Are you engaging your occupational therapist for assessment of depression risks? Are your physical and speech therapists receiving referrals for cognitive decline and reduced physical activity, both of which are risk factors for depression and resulting factors when changes in mood occur?
Once mood changes are identified, are the appropriate professionals informed with care plans implemented to address risk factors above?
Let’s face it, while a slow and gradual reopening may take place across the nation, we will continue to have many seniors in our homes isolated for a longer period of time.
Don’t let their kindness and smiling faces mask their sadness.
Dig deep, assess the unique coloring in the heaviness, and understand what may be just below the surface.
Renee Kinder, MS, CCC-SLP, RAC-CT, is Executive Vice President of Clinical Services for Broad River Rehab and a 2019 APEX Award of Excellence winner in the Writing–Regular Departments & Columns category. Additionally, she serves as Gerontology Professional Development Manager for the American Speech Language Hearing Association’s (ASHA) gerontology special interest group, is a member of the University of Kentucky College of Medicine community faculty, and is an advisor to the American Medical Association’s Relative Value Update Committee (RUC) Health Care Professionals Advisory Committee (HCPAC).





