


I am constantly reminded how the complexities of nature astound me. Recently, I became aware of the impending cicada invasion that will happen this year in various regions of the United States.
According to the University of Connecticut Periodical Cicada Information Pages, in certain parts of the country, 2024 will be a special year for periodical cicadas for the following reasons:
- For the first time since 2015, a 13-year brood will emerge in the same year as a 17-year brood.
- For the first time since 1998, adjacent 13- and 17-year broods will emerge in the same year.
- For the first time since 1803, Brood XIX and XIII will co-emerge.
- You will be able to see all seven named periodical cicada species as adults in the same year, which will not happen again until 2037.
- You will not see all seven named species emerge in the state of Illinois again, for example, until 2041.
Wow! Get ready for some noise. Some of us had better think before we go barefoot and have plenty of windshield wiper fluid handy, if you know what I mean.
As this imminent event gets closer, it got me thinking about the complexities of the minimum data set. I hope you realize just how intricate a dance it is to get one completed, on time, accurately and with adequate supporting documentation.
Not to be taken for granted, this task requires a specific skill set. I hope you appreciate your MDS coordinator(s). Those who are successful work hard at getting this right. Consider that a single MDS influences care planning, quality reporting, Five-Star rating, reimbursement and survey success. These are not trivial matters.
For context, take a look at the color-enhanced example below. You will notice that a single portion of one section of the MDS can impact every one of these areas. Completing an MDS is like dropping a pebble in a pond. The ripple effects are significant.
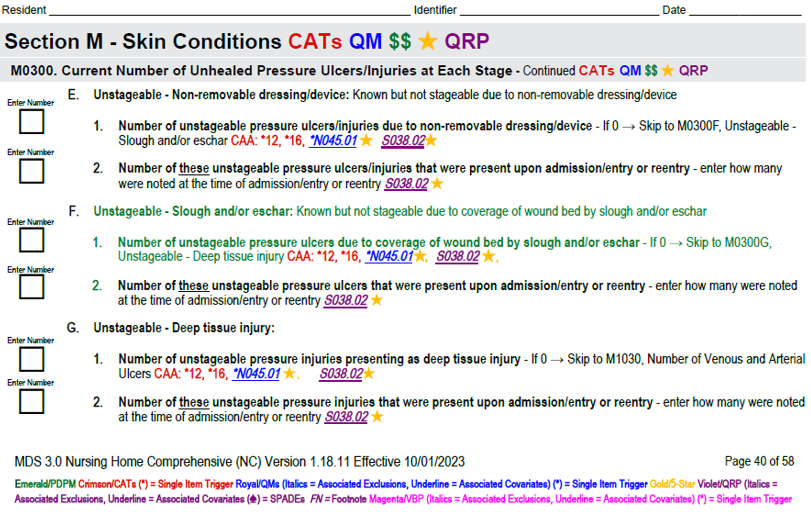
Let’s break it down.
Care plans are a complex distillation of the information gathered on a comprehensive MDS assessment. This 58-page document requires a significant amount of time and resources to complete accurately. Reevaluation is required on an ongoing quarterly basis and with significant changes in resident status.
From the information gathered on this assessment, there are 20 potential detailed Care Area Assessments (CAAs) and other assessments that must be completed. CAA data, coupled with other information, results in a resident-centered care plan that guides resident care.
Quality reporting is a complicated array of measures that have an impact on the following four important programs to which providers must pay attention.
- IQIES facility and resident level reporting (18 MDS-based measures)
- Five-Star rating (9 MDS-based measures)
- Skilled Nursing Facility Quality Reporting Program (SNF QRP) (8 MDS-based measures)
- Value-Based Purchasing Program (SNF VBP) (2 MDS-based measures by 2028).
Each of these quality measurement programs is driven, in part or in whole, by MDS-based quality measures. There are also several state Medicaid systems that rely on quality measurement for add-ons to their Medicaid rates.
Reimbursement systems, both state and federal, rely on information collected on the MDS to generate acuity indexes that inform payment. This is not new. However, due to the elimination of Section G along with other revisions that came with the implementation of MDS 3.0 v1.18.11 last October, many states have switched from a RUGs-based CMI calculation to one that uses PDPM instead.
In order to continue with a RUG-based CMI rate calculation, there are some states that have opted not to transition to PDPM immediately. Those states require their MDS coordinators to complete an extra assessment, called the Optional State Assessment (OSA), along with the other required assessments,
Survey success relies heavily on timely, accurate and compliant MDS completion. The excerpt below represents F-tags associated with the MDS process detailed in the State Operation Manual Appendix PP. This 863-page behemoth contains interpretive guidance for surveyors.
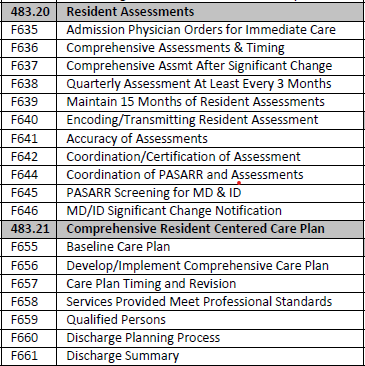
These 18 F-tags are those under which citations can be made specifically for non-compliance with the MDS and care planning processes. However, there are myriad other tags where a connection can be made to MDS and Care plan non-compliance where other citations can occur.
What does this all mean?
Much more could be said about the complex nature of the MDS and the wide-ranging impact that it has. The point of this missive is simply a reminder that the individuals who complete these assessments are extraordinary people. The initial view that consumers and federal agencies have of your facility relies much on their skill.
Granted, the processes associated with MDS completion are interdisciplinary. But it takes the MDS coordinator to manage them. Timeliness, accuracy and compliance aren’t spontaneous. They don’t “just happen.”
While the coming cicada invasion of the summer of 2024, with all its rarity, complex harmonization and environmental impact, will be a once-in-a-lifetime event, one has to consider that the complex coordination that must happen for a successful, accurate and compliant MDS occurs every day.
The value that a qualified MDS coordinator brings to the table simply cannot be overstated. Absent that, I’ve seen the destructive downside ripple effect.
Here, I’m reminded of one of my favorite quotes. Henry David Thoreau said it this way: “Our least deed, like the young of the land crab, wends its way to the sea of cause and effect, as soon as born, and makes a drop there to eternity.”
Cicada swarms of biblical proportion or skilled MDS coordinators, the effects can be incredible.
This summer, if you happen to experience the expected insect incursion and your windshield wipers are doing their job, think about how fortunate you are if you have an MDS coordinator who knows their stuff. Make sure they have the tools they need to succeed, and then watch the unmistakable ripples grow.
Joel VanEaton, BSN, RN, RAC-CT, RAC-CTA, is a master teacher and the executive vice president of PAC Regulatory Affairs and Education at Broad River Rehabilitation. For further inquiries, he may be contacted here.
The opinions expressed in McKnight’s Long-Term Care News guest submissions are the author’s and are not necessarily those of McKnight’s Long-Term Care News or its editors.
Have a column idea? See our submission guidelines here.





