


I’m a sucker for classic movies. My parents made sure I grew up watching black and whites of the likes of Fred Astaire, Ginger Rogers, Bing Crosby, Danny Kaye, Rosemary Clooney, Gene Autry, John Wayne, Cary Grant and so many more like them.
Sadly, not many movies are made like those anymore. I recently watched Cary Grant in “An Affair to Remember.” It’s a great flick, even if it is in color, and if you plan to watch it, have a box of tissues handy.
In this movie, Carry Grant’s character, Nickie, and the female lead’s character, Terry, meet on a cruise. They fall in love and plan to meet six months after they return to the States at the top of the Empire State Building in New York City to get married.
Recently, the Centers for Medicare & Medicaid Services released the FY 2025 SNF PPS proposed rule and boy, are there some memorable items that CMS threw in there for our consideration.
A Request for Information, or RFI, to remember from this proposed rule, one that will require our participation and comment, is related to CMS’ rethinking the NTAs.
CMS is requesting feedback on their 2019 final rule promised revisit of the NTA category.
Notable RFI considerations
Among the notable considerations, CMS would update study population and will, instead of the original pre-PDPM cohort, use Medicare Part A SNF stays with admissions from FY 2019 through FY 2022.
CMS is also considering making certain methodological changes to reflect more accurate and reliable coding of NTA conditions and extensive services on SNF Part A claims and the MDS after PDPM implementation and would use that data exclusively as much as possible.
Finally, CMS is considering prioritizing the reporting and selection of conditions on the MDS by raising the cost threshold for selecting any overlapping conditions found in other sources from any additional cost to five dollars in average NTA cost per day. This is the amount that is observed to be generally associated with a one-point NTA increase.
What does this mean?
Based on this revised methodology, CMS is seeking feedback on the resulting alterations to the familiar NTA list of conditions and extensive services currently found in Chapter 6 of the RAI Manual and CMS’ PDPM website NTA fact sheet.
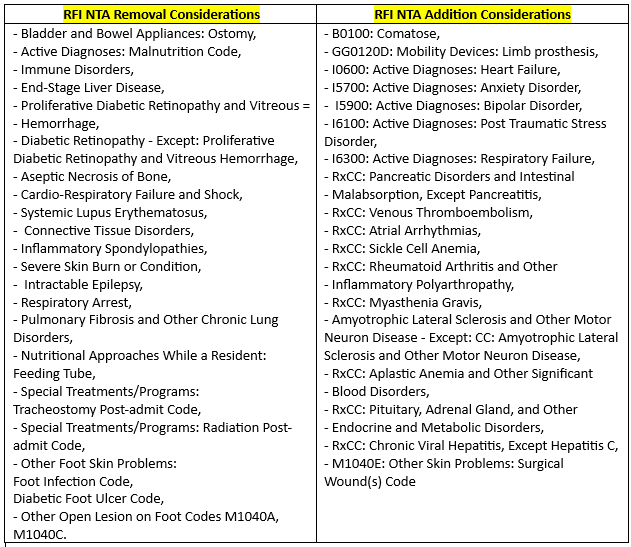
When I say alterations, I mean a complete makeover. With these changes there are 16 familiar NTAs that would be removed and 17 new/revised NTAs that would be added for a resulting grand total of 50 NTAs.
In addition, several point values would shift as well. Nine retained NTAs would decrease in point values, some significantly. For example, Special Treatments/Programs: Ventilator or Respirator Post-admit Code would be revised from four points to one point and Section K: Parenteral IV Feeding: Level High would be revised from seven points to five.
Conversely, there would be four retained NTAs with point values that increase. For example, Lung Transplant Status is would be revised from three points to five, and Cystic Fibrosis would be revised from one point to three.
The table below is a summary of the additions to and subtractions from the NTA list that CMS is asking us to comment on.
Back to the basics
As you know, the NTA component utilizes a comorbidity score to assign the patient to an NTA component case-mix group, which is determined by the presence of conditions or the use of extensive services that were found to be correlated with increases in NTA costs for SNF patients.
Yes, things have changed since 2019 and the MDS data now reflects more accurately the use of these services. But take a look at the list of NTAs that are being considered for the discard pile: feeding tubes, malnutrition, diabetic foot ulcers, tracheostomy and diabetic retinopathy, to name a few.
The research and methodology changes may point in that direction, but we still get those patients. The points associated with these conditions are valuable and represent the real PDPM dollars required to care for them.
How should we respond?
In a recent Open Door Forum and at the AAPACN National Conference, CMS’s John Kane made it clear that these revisions are presently only part of an RFI.
I believe him. We are not married to these yet. However, the extensive research and methodology change that resulted in these suggested changes make this feel more like a proposal than an RFI.
May 28th is the deadline for comments. I plan to get my two cents worth on the table. I hope you do as well.
The final RFI affair
In an “Affair to Remember,” Terry is involved in a serious accident while on her way to the Empire State Building. The resulting injury renders her unable to walk, and as such, she believes the relationship to be over.
Nickie waits at the Empire State Building and when Terry doesn’t show up, he fears that she has married or does not love him anymore. He eventually takes up a long-lost passion for painting and life appears to go on, sadly.
A chance encounter some months later proves their fears wrong. Their final meeting is a beautiful scene. The film ends with the two in a passionate embrace as Terry says to Nickie, “If you can paint, I can walk. Anything can happen, don’t you think?”
It’s possible these NTA changes will evaporate or be revised between now and when CMS intends to resolve the RFI. Just remember last year when the CORE Q did not come to fruition or when we saw positive revised PDPM ICD-10 mapping.
CMS is listening. Let’s be sure our voices are heard.
Anything can happen, don’t you think?
Joel VanEaton, BSN, RN, RAC-CT, RAC-CTA, is a master teacher and the executive vice president of PAC Regulatory Affairs and Education at Broad River Rehabilitation. For further inquiries, he may be contacted here.
The opinions expressed in McKnight’s Long-Term Care News guest submissions are the author’s and are not necessarily those of McKnight’s Long-Term Care News or its editors.
Have a column idea? See our submission guidelines here.




