


EDITOR’S NOTE: For the new column on this topic, with all up-to-date observations, newly appearing Nov. 28, 2022, click here.
So much is being written recently about the current trends that many are seeing with regard to the PDPM [Payment Driven Payment Model]. Early predictions warned about significant reductions to the amount and type of therapy provided and how that reality would draw the attention of CMS [Centers for Medicare & Medicaid Services]. In part that has come true. We have all seen the stories and testimonials of reductions in therapy provisions. And CMS, true to its word, is looking. You may get an opportunity to know your Unified Program Integrity Contractor, or UPIC, up close and personal.
However, some recent indications are that the general trend is not as dire as was first predicted. Some now feel that the overall industry turn to the PDPM did not take as dramatic a shift as was predicted. Rather, some now seem to indicate that the reductions in therapy services and increases in group and concurrent therapy are slight enough to warrant neither significant scrutiny from CMS nor an imminent major correction to the non-budget neutral payment structure. Who knows? Your personal experience in your SNF will tell a specific tale and the FY 2021 Proposed Rule, due out this spring, will certainly give us more of a reality check.
A game called SPADEs
With that said, as we wait for more, it’s time to be turning our collective attentions to what we already know will be part of our FY 2021 reality, namely a new game we will all be learning called SPADEs. With the publication of the FY 2020 final rule and the posting of the DRAFT MDS data set v1.18.0 with the associated change history document, it has become clear that in addition to adjusting to whatever CMS decides to do related to the PDPM this fall, we most certainly will have to accommodate SPADEs.
SPADEs is an acronym for Standardized Patient Assessment Data Elements. Required by the IMPACT Act, SPADEs are elements that will be required to be reported in each of the post-acute are setting assessment tools (MDS, IRF PAI, OASIS and LCDS), and will significantly reshape these tools. The QRP is a residual of IMPACT, Section GG, Falls with Major injury and Pressure Ulcers New or Worsening were the first QRP measures to contain SPADEs. The goals of implementing cross-setting SPADEs are to facilitate care coordination and interoperability and to improve Medicare beneficiary outcomes. Another key aim is cross setting comparisons and referral placement. You will have to look good compared to your Post-Acute care competitors. In short, the changes coming to the MDS this fall are the biggest change to MDS 3.0 since MDS 3.0. The comprehensive assessment is growing by 10 pages to 61. Now is the time to begin familiarizing yourself with these new data elements.
In the FY 2020 Final Rule, CMS finalized new standardized patient assessment data elements, or SPADEs, to be reported with SNF admissions and discharges for five categories specified in the IMPACT Act; Cognitive function (e.g., able to express ideas and to understand normal speech)
and mental status (e.g., depression and dementia); Special services, treatments and interventions (e.g., need for ventilator, dialysis, chemotherapy and total parenteral nutrition); Medical conditions and co-morbidities (e.g., diabetes, heart failure and pressure ulcers), Impairments (e.g., incontinence; impaired ability to hear, see, or swallow); Other categories as deemed necessary by the secretary.
In order to get ahead of the curve, download a copy of the DRAFT data set. Getting a handle on the changes to this document now will serve you well as we move through the proposed and final rulemaking process and the inevitable publication of the significantly revised RAI manual. The changes to the MDS data set due to the addition of SPADEs are significant. SPADEs have been added to all federally required assessments, PPS as well as OBRA, and even Section A has been revised in the OSA. As you may have heard, Section G has been replaced by section GG in all federally required assessments and section Q has had a much-needed update.
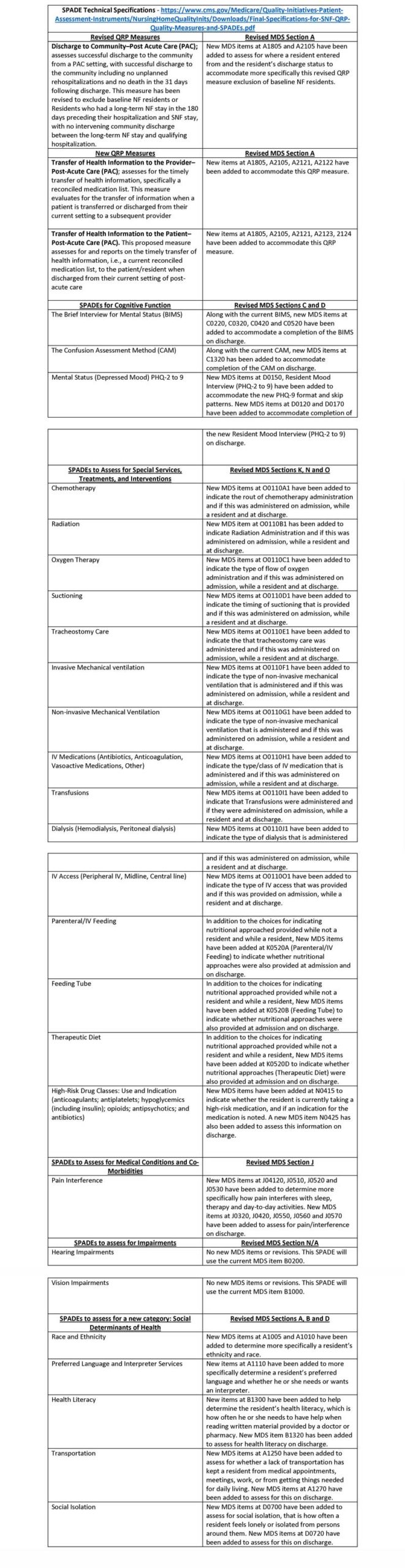
So just what are the SPADEs and how has the MDS changed? The tables below review the new and revised QRP measures as well as each SPADE along with the the MDS items affected by these additions. Have your copy of the DRAFT data set handy as you review these changes. Context is key and will help you get a sense of the scope of the actual revisions.
Quality measures
Also, as you consider these updates, consider the following implications. With the removal of section G, not only will states need to consider alternatives to their case mix calculations, CMS will need to revise the technical specifications for the following quality measures:
- Short Stay – Percent of Residents or Patients with Pressure Ulcers That are New or worsened, Percent of Residents Who Made Improvement in Function.
- Long Stay – Percent of High-Risk Residents with Pressure Ulcers, Percent of Residents Whose Need for Help with ADLs has Increased, Percent of Residents whose Ability to Move Independently Worsened, Percent of Low Risk Residents Who Lose control of Their Bowel or Bladder.
- Claims Based Measures – Residents who Were Re-Hospitalized after a Nursing Home Admission, Number of hospitalizations per 1,000 Long-Stay Resident Days, Residents Who Had an Outpatient ED Visit, Number of Outpatient ED Visits per 1,000 Long-Stay Resident Days.
CMS will also need to update 17 of the current 20 CAAS that will also be affected: - CAA 1 – Delirium, CAA 2 – Cognitive Loss/Dementia, CAA 4 – Communication, CAA 5 – Activity of Daily Living (ADL) Functional/Rehabilitation Potential, CAA 6 – Urinary Incontinence and Indwelling Catheter, CAA 7 – Psychosocial Well-Being, CAA 8 – Mood State, CAA 10 – Activities, CAA 11 – Falls, CAA 12 – Nutritional Status, CAA 14 – Dehydration/Fluid Maintenance, CAA 15 – Dental Care, CAA 16 – Pressure Ulcer/Injury, CAA 17 – Psychotropic Medication Use, CAA 18 – Physical Restraints, CAA 19 – Pain, CAA 20 – Return to Community Referral.
The takeaway: SPADEs are here to stay. CMS is already considering future SPADEs and QRP measures as well. So, stay tuned to what may or may not happen with the PDPM this fall. But start now and get up to speed with SPADEs. The revised data set will be here in a few short months. Don’t wait to become a pro. You don’t want to lose at this game.
Joel VanEaton, BSN, RN, RAC-CT, is the VP of compliance and regulatory affairs at Broad River Rehab.





