


Good things do come in threes, especially if we are talking about Mary Ousley, Dava Ashley and David Grabowski — three industry mavericks who have contributed to U.S. eldercare in countless ways. It is my great fortune not only to know these three extraordinaires, but to have brought them together for a recent panel discussion at LTC 100.
The panel was titled “SNF Regulatory and Reimbursement Forecast.” It was a perfect topic to discuss as we exit the COVID-19 pandemic (hopefully), transition to new governmental leadership, and respond to the proposed rule. I’d like to share a sampling of the discussion by focusing on just three topics, each with three comments by these industry devotees.
David C. Grabowski, PhD.,. is professor of healthcare policy at Harvard Medical School’s Department of Health Care Policy; Mary Ousley, RN, is chief strategy officer for long-term care at PruittHealth and the 2021 McKnight’s Women of Distinction Lifetime Achievement Award winner; and Dava Ashley, MBA, is president of Covenant Care. The paragraphs below are not direct quotes, but rather themes gleaned from our hour-long panel.
The Biden Administration
Dava: The administration is vested in health equity, but that must come with better accounting for social determinants of health (SDOH). There are unique challenges, clinical and otherwise, in caring for the dual-eligible population — we saw them firsthand with COVID-related illness and vaccination acceptance. We must be prepared to address these challenges. This administration must commit to accounting for these SDOH as they construct measures that sanction or reward us. A provider cannot be penalized for caring for the people who are most in need.
David: The interim final rule is a great example of the value this administration places on transparency. Providers are now required to report resident/patient and staff vaccination rates, which is tremendously helpful for residents and families. However, it also represents a tremendous reporting burden; CMS should work to lessen that burden or pay facilities for undertaking it. Another example of the administration’s focus on transparency is outsider money, which is an issue that has exploded as of late. There is suspicion, and now extreme scrutiny, around private equity and other outsider investors. The administration has promised more financial transparency and accountability, plus measures to crack down on any kind of questionable related-party transactions. Many states are leading on this issue, putting policy in place to increase financial transparency.
Mary: The $400 billion earmarked for home- and community-based services (HCBS) is interesting. There are 800,000 people on the waiting list for Medicaid. These funds are directed toward these individuals, and likely there will be spillover to nursing homes. This is not a competition between HCBS and skilled nursing; it’s complementary. We must further develop skilled nursing to include infection preventionists in every building and registered nurses around the clock. As a profession, we must establish what is the right thing to do and let policy follow. $15 million would accomplish this, and relatively speaking, that’s not a lot of money.
Reimbursement/Compliance
Mary: In reading the proposed rule, I don’t refer to the $1.7 billion as overpayment. CMS is not accounting for the “real cost of COVID.” You must cross-reference every bit of CDC guidance and the cost of care associated with it to truly see the financial impact of COVID — especially early on when every admitted resident was to be treated as if they were COVID positive, and they were coming in much more acute. How do we attribute the $1.7 billion to the cost of care? CMS attempted, but did not go far enough. The cost of isolation, both physical and emotional, and PPE are just some examples. Keep in mind that this rule is not written in ugly language; it’s reasonable and collaborative. That’s hopeful.
Dava: Thinking about compliance and the first PDPM PEPPER report, I like to remind people that PEPPER is the end of the process. You must have compliance processes in place within your organization to ensure that the clinical documentation supports patients’ needs. Multiple layers to ensure compliance are required. Compliance checks should occur both in real time and then again at triple check. We then add yet another layer and have external compliance auditors to double check the checkers. Be proactive, then let the PEPPER report tell the positive story. I do wonder how COVID will impact current and future PEPPER measures. We were admitting patients who were much sicker than usual, and they went directly into isolation. Certainly, that impacted the delivery of care and subsequent outcomes.
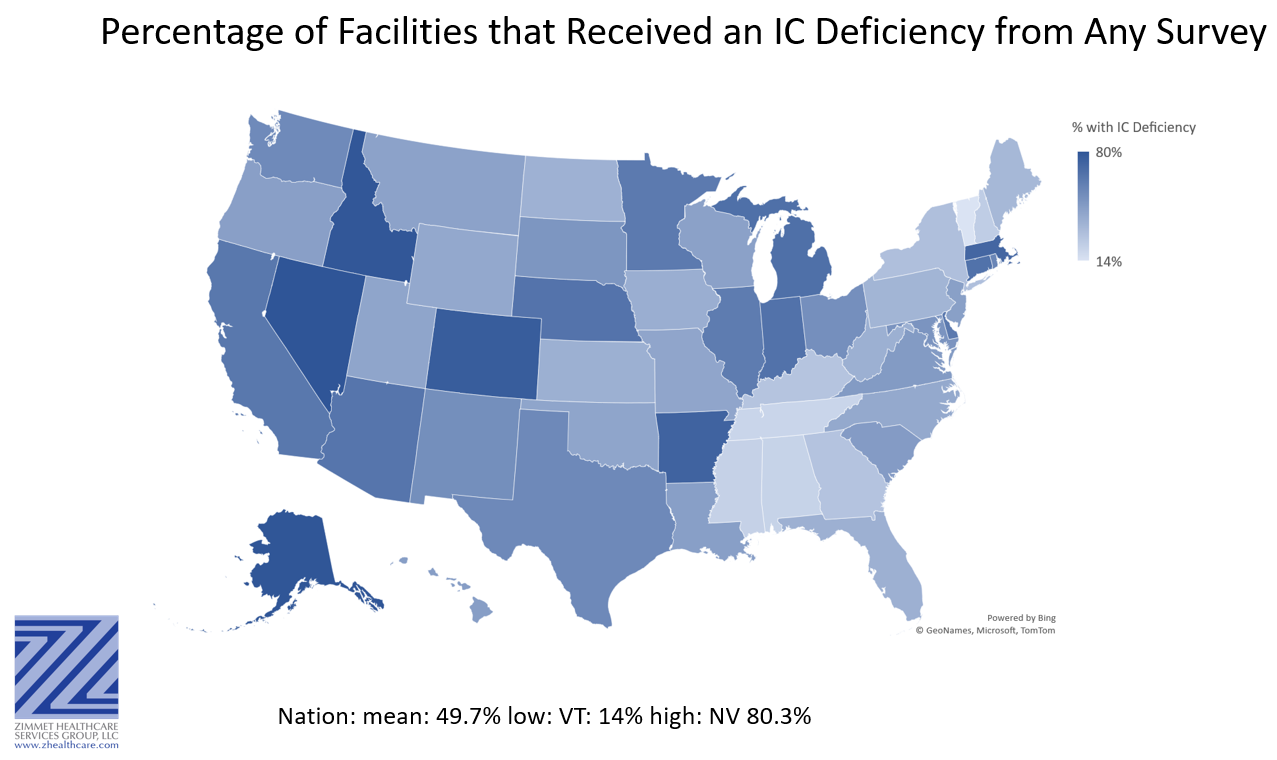
David: Responding to the map that illustrates the disparate state averages of infection control deficiencies: Despite the Coronavirus Commission’s recommendations for PPE, rapid testing, more resources for staff, and other topics, CMS more fully embraced additional infection control investigations. CMS needed a villain, and it was not enough to say the villain was COVID. Our own research, plus that of others at Brown and the University of Chicago, suggested that all facilities were susceptible to COVID. This was not a bad-actor outcome — all facilities needed help. However, that message did not allow CMS to put their finger on a villain, so they villainized the industry. This does not get us to where we need to be in terms of better infection control, for example.
Breaking the Cycle
Dava: We must break the cycle of demonizing nursing homes. [See the New York Times’ recent scathing rebuke on our industry; while no one in our profession claims to be perfect, a previous blog of mine discussed the inaccuracy of the piece’s arguments.] Focus on clinical care and on patient and resident satisfaction. Many of these folks have no other place to go. They turn to us, and we are there for them. We must tell the story. Help those who can go to lower care settings and continue to help those who are not able.
Mary: “The beatings will continue until morale improves.” Let’s look at the regulatory process. The regulatory (survey) experience depends, to a great extent, on which state a facility resides in. With over 753 pages of regulations and interpretive guidelines, nursing homes in this nation are 92% compliant with all these requirements. On average, a nursing home receives eight deficiencies per survey, meaning they are 92% compliant. If we could reverse the language, it would make a huge difference.
David: Deficiencies are not about quality improvement or quality assurance. We absolutely need a system-wide approach to address some of the challenges, but more survey/regulation is not the answer. I worry a lot about some of the measures in the proposed rule, such as healthcare-associated infections (HAI). This is a really challenging measure to risk adjust, which the rule acknowledges.
The more things change …
Despite everything real or imagined, none of the mighty three on the LTC 100 panel felt that the industry would be allowed to fail. We did acknowledge that there would likely be significant closures of nursing homes — perhaps as much as 20% — over the next year and beyond, and that the industry landscape might look very different than what exists today. However, the consensus was clear: Skilled nursing facilities and nursing homes are vital to our society. Whatever we become, we will continue to fulfill an essential need and contribute to the well-being of our nation’s elders.
Steven Littlehale is a gerontological clinical nurse specialist and chief innovation officer at Zimmet Healthcare Services Group.




